

Health Data Analysis for Improving Breast Cancer Screening
Note: The following project represents a hypothetical academic exercise. It does not reflect work endorsed by the representative brand.
For our Health Data Science course, Alexa Water & I worked together to explore the vital roles of data, information, and information systems in the implementation and evaluation of Population Health initiatives and Value-based Care initiatives.
Selecting an ACO for our analysis.
We picked Bayview Physicians Group (‘Bayview’), a small ACO, to analyze and a larger ACO, Duke Connected Care, LLC, to compare.

Framing Questions
How do Bayview and Duke ACOs compare
breast cancer screening, key demographics, and cost savings?What successful cancer screening initiatives at Duke should Bayview seek to implement?

Understanding Demographics
Bayview (Chesapeake, VA) serves ~20,000 beneficiaries from southeastern VA and northeastern NC, whereas Duke (Durham, NC) serves ~50,000 beneficiaries from north-central NC. However, Duke cares for over twice as many beneficiaries as Bayview, and Duke’s population may face higher social needs that are greater % minority groups and greater % dual-eligible.

Data
We considered the following data fields to fit our analysis best: Number of beneficiaries (N_AB), Breast cancer screening rate (ACO20), Colon cancer screening rate (ACO19), PCP visits (P_EM_PCP_Vis), and consider including SDOH measures: % Non-white (calculated), Poverty rate, % Dual eligible.



Breast cancer screening is a key quality measure ripe for improvement at Bayview. Nearby Duke ACO has demonstrated improved breast cancer screening rates…
Despite caring for a larger population that may have more complex social needs
Despite decreases in primary care visits and the onset of a pandemic
All while improving cost savings
What successful cancer screening initiatives at Duke should Bayview seek to implement?
What is Duke doing better?
Duke is doing better at breast cancer screening despite caring for a larger population and complex social needs, decreasing PCP visits due to the pandemic, and improving its cost savings. So, what initiates are making Duke successful at cancer screening that Bayview should seek to implement?
We did a little research to determine why Duke’s cancer screening rate was high. From 2010 to 2015, the Duke Cancer Institute and the Office of Health Equity and Disparities (OHED) engaged in a coordinated effort to improve community health and address health disparities.
Duke Strategies & Initiatives in Cancer Screening
They implemented five strategic step process:
Create an engaged and diverse community advisory council that offers diverse perspectives across the cancer spectrum.
Conduct a robust community health needs assessment and share findings, i.e., they conducted focus groups and analyzed both quantitative and qualitative data.
Establish program and research priorities: The OHED analyzed the findings to give recommendations and improve the previous Duke Cancer Institute programs, services, research, or collaborations with key partners to address specific priorities and goals.
Develop or enhance partnered programming and research aligned with priorities: The OHED increased its capacity to implement community and patient programming.
Evaluation and outcomes: the OHED programs and activities kept evaluating and modifying processes and impact outcomes to ensure met goals and objectives.
All this improved their breast cancer screening rate. Here are the statistics from the 2019 Annual report:
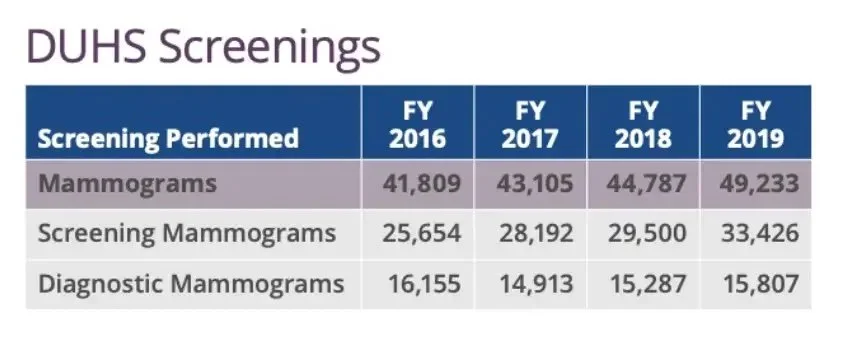
So these are the four key programs that made a significant impact on Duke’s cancer screening:
Patient navigation program:
Community screening programs & faith initiatives
Outreach program:
Diversity & inclusion program
Recommendations
So putting together our research and analysis, our recommendation for Bayview was to:
Re-evaluate current breast cancer screening initiatives in the patient population at Bayview. Are initiatives targeting patients most in need or the care gap?
Engage with the community and stakeholders to develop patient navigation and outreach programs.
Maintain a focus on diversity and inclusion in the workforce, training, and community outreach.
References:
ACO Data from https://data.cms.gov/search?keywords=aco&sort=Relevancy
Centers for Medicare & Medicaid Services. (2020). Performance Year Financial and Quality Results. Medicare Shared Savings Program. https://data.cms.gov/medicare-shared-savings-program/performance-year-financial-and-quality-results
Office of Disease Prevention and Health Promotion. (2014). Objective C17: Increase the proportion of women who receive breast cancer screening based on the most recent guidelines. HealthyPeople.Gov. https://www.healthypeople.gov/node/4055/data_details
Barrett N. J., Hawkins T. V., Wilder J. W., et al. (2016). Implementation of a Health Disparities & Equity Program at the Duke Cancer Institute. https://www.accc-cancer.org/docs/documents/oncology-issues/articles/2003-2016/2016/so16/so16-implementation-of-a-health-disparities-equity-program-at-the-duke-cancer-institute.pdf?sfvrsn=388f90f0_11
Duke’s Annual Report 2019 — http://dukecancerinstitute.org/news/dci-fy2019-annual-report-published